This post was created in partnership between AMSA’s Global Health Action Committee and AMSA Partner Canopy Learn.
“No puedo respirar,” she said at the other end of the phone line. Lucia’s son would normally accompany her to primary care visits to act as a translator. However, the COVID-19 pandemic made this impossible. “Can you call an interpreter?” the physician asked the staff in the office as he shuffled papers around. The dark bags under his eyes gave away the exhaustion; exhaustion from too many sick patients, too little time, too many shortages. There was a climate of frustration, distress, and helplessness in the office. It was evident that the COVID-19 pandemic had brought to the surface not only the vast racial inequalities that plague our health system but also the deeply concerning barriers of caring for patients with Limited-English Proficiency (LEP).
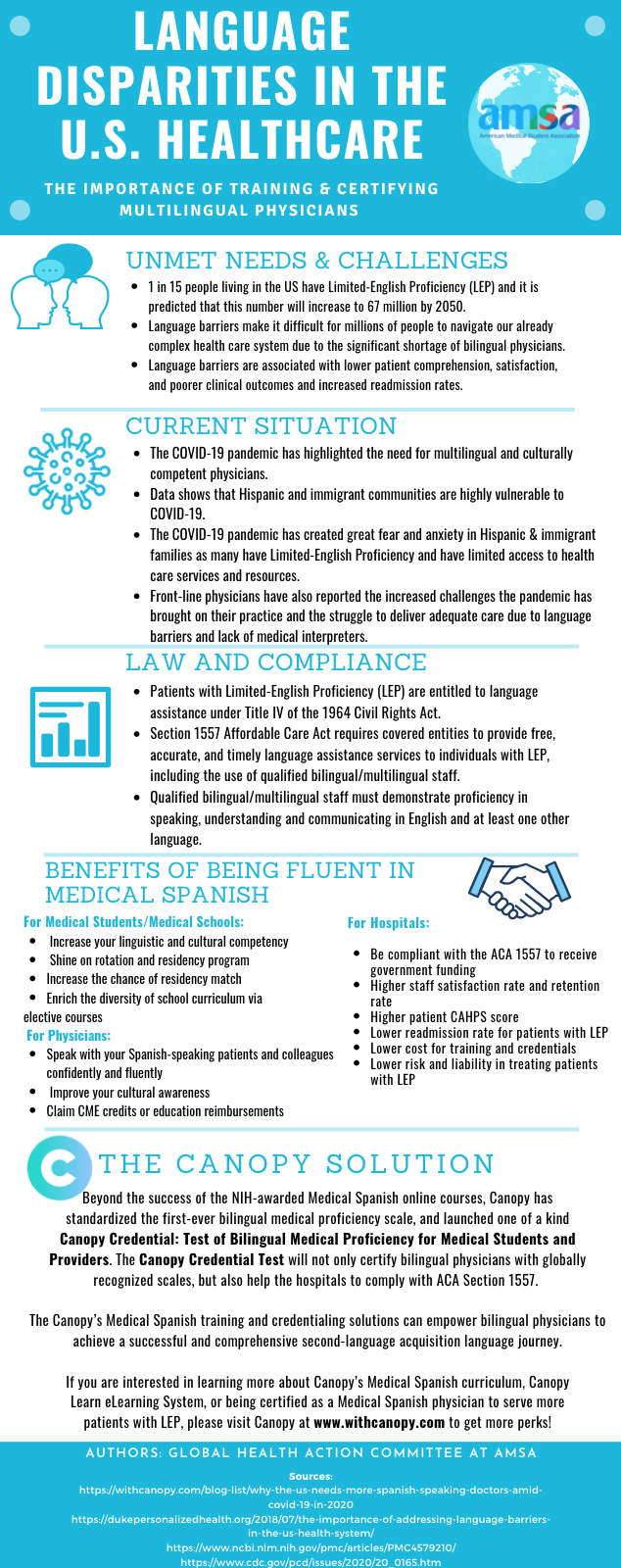
Lucia is one of the 20 million people living in the U.S with limited English proficiency. According to the Journal of General Internal Medicine it is predicted that this number will increase to 67 million by 2050. According to Jill Wilson, a senior research analyst in the Metropolitan Policy Program, 66 % of the U.S LEP population speaks Spanish. Asian and Pacific island languages make 18.4 %, Indo-European languages make 11.9 %, and 3.4 % include other languages such as Arabic, African, and Native American.
Language barriers make it difficult for millions of people to navigate our already complex healthcare system due to the significant shortage of medical interpreters and bilingual physicians. This significant shortage translates to a subpar delivery of care to patients with LEP and in the context of the COVID-19 pandemic it often becomes one of the biggest barriers in a life-or-death situation. Multiple research studies have revealed that language barriers are associated with lower patient comprehensions, satisfaction, and poorer clinical outcomes and increased readmission rates.
Due to the vast array of people that have Limited-English Proficiency (LEP), it is imperative that providers are able to accommodate these individuals so that they may deliver the best medical care possible. Patients with LEP are entitled to language assistance under Title IV of the 1964 Civil Rights Act. Additionally, Section 1557 Affordable Care Act requires covered entities to provide free, accurate, and timely language assistance services to individuals with LEP, including the use of qualified bilingual/multilingual staff. Qualified bilingual/multilingual staff must demonstrate proficiency in speaking, understanding and communicating in English and at least one other language. Unfortunately, there is often a shortage of staff able to provide these vital sources for LEP patients, and thus it is imperative that providers can communicate with these individuals.
Beyond the success of the NIH-awarded Medical Spanish online courses, Canopy has standardized the first-ever bilingual medical proficiency scale, and launched one of a kind Canopy Credential: Test of Bilingual Medical Proficiency for Medical Students and Providers. The Canopy Credential Test will not only certify bilingual physicians with globally recognized scales, but also help the hospitals to comply with ACA Section 1557. The Canopy’s Medical Spanish training and credentialing solutions can empower bilingual physicians to achieve a successful and comprehensive second-language acquisition language journey. If you are interested in learning more about Canopy’s Medical Spanish curriculum, Canopy Learn eLearning System, or being certified as a Medical Spanish physician to serve more patients with LEP, please visit Canopy at www.withcanopy.com to get more perks! Learn more about AMSA member benefits with Canopy here.